Most families touring assisted living communities focus on room size, staffing ratios, and activity programs. Food barely makes the list. But the role of nutrition in assisted living reaches far beyond three meals a day. It shapes whether your loved one maintains muscle, recovers from illness, stays mentally sharp, and feels connected to the people around them. This guide breaks down what actually happens with nutrition inside these communities, what the regulations require, what clinical care looks like versus a standard dining program, and exactly what you should be asking before you sign anything.
Table of Contents
- Key takeaways
- The role of nutrition in assisted living for seniors
- Regulatory standards guiding nutrition services
- Meals as social medicine
- What families and caregivers should do
- Challenges in nutrition care that are rarely discussed
- My perspective on what families consistently miss
- How Assistedlivingadvisers can help you find the right community
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Nutrition goes beyond meals | Clinical nutrition care and general dining services are two separate things with different staff, standards, and outcomes. |
| Protein needs increase with age | Seniors require 1.0–1.2 g of protein per kilogram of body weight daily to prevent muscle loss. |
| Malnutrition is widespread | An estimated 35–50% of seniors in long-term care are malnourished, making active monitoring non-negotiable. |
| Social meals protect health | Shared mealtimes reduce isolation and directly improve appetite, mood, and overall nutrition status. |
| Families must advocate | Ask specifically whether a Registered Dietitian Nutritionist reviews individual resident care plans, not just facility-wide menus. |
The role of nutrition in assisted living for seniors
Aging changes how the body processes food at nearly every level. Metabolism slows, appetite decreases, gut absorption weakens, and the sense of taste and smell dims. These changes mean that eating less food while needing more nutrients creates a collision that many seniors quietly lose.
Protein and muscle mass
Seniors require 1.0–1.2 grams of protein per kilogram of body weight daily. That is meaningfully higher than what younger adults need, and it exists for one reason: preventing sarcopenia, the age-related loss of muscle mass that drives falls, frailty, and loss of independence. A 150-pound woman needs roughly 68–82 grams of protein every single day just to hold ground.
Micronutrients that matter most
The following nutrients become critically important as the body ages and absorption rates decline:
- Vitamin B12: Absorption drops with age due to reduced stomach acid; deficiency causes nerve damage and cognitive decline
- Calcium and vitamin D: Both work together for bone density and fall prevention; vitamin D also supports immune function
- Magnesium: Supports muscle and nerve function, often depleted by diuretics commonly prescribed to older adults
- Omega-3 fatty acids: Linked to reduced inflammation and better cognitive function in aging populations
Hydration and its hidden risks
Older adults have a diminished sense of thirst, which makes voluntary hydration unreliable. Dehydration in seniors contributes directly to urinary tract infections, cognitive fog, and fatigue. A practical baseline target for adults over 65 with low to moderate activity is half their body weight in ounces of water per day. A 160-pound man, for example, should be drinking around 80 ounces daily. Assisted living communities that track hydration systematically are doing something genuinely protective for their residents.

Regulatory standards guiding nutrition services
Understanding the rules behind assisted living nutrition helps you evaluate what a facility is actually required to provide versus what they choose to offer.
Here is how the regulatory framework typically plays out:
- Meal frequency requirements: Most states mandate a minimum of three meals per day with snacks available, structured around adequate caloric intake.
- Menu review cycles: Assisted living meal plans follow 4–6 week rotating menus reviewed by Registered Dietitian Nutritionists for macro and micronutrient balance per the Dietary Guidelines for Americans.
- Therapeutic diet accommodations: Facilities must accommodate physician-ordered diets including low-sodium, diabetic, renal, and texture-modified preparations.
- Weight monitoring: Unintentional weight loss exceeding 5% in 30 days triggers a clinical review and required intervention under regulatory guidelines.
- Dysphagia management: Approximately 15% of older adults have dysphagia, requiring texture-modified diets standardized through the IDDSI framework to prevent aspiration pneumonia.
RDNs vs. nutritionists: why the distinction matters
Registered Dietitian Nutritionists hold advanced degrees, complete supervised clinical internships, and pass national board exams. The title “nutritionist” is unregulated in most states. Anyone can call themselves one. When you are asking about nutrition staff at a facility, you want to know whether a credentialed RDN reviews individual resident care plans, not just the general menu. Those are very different levels of involvement.
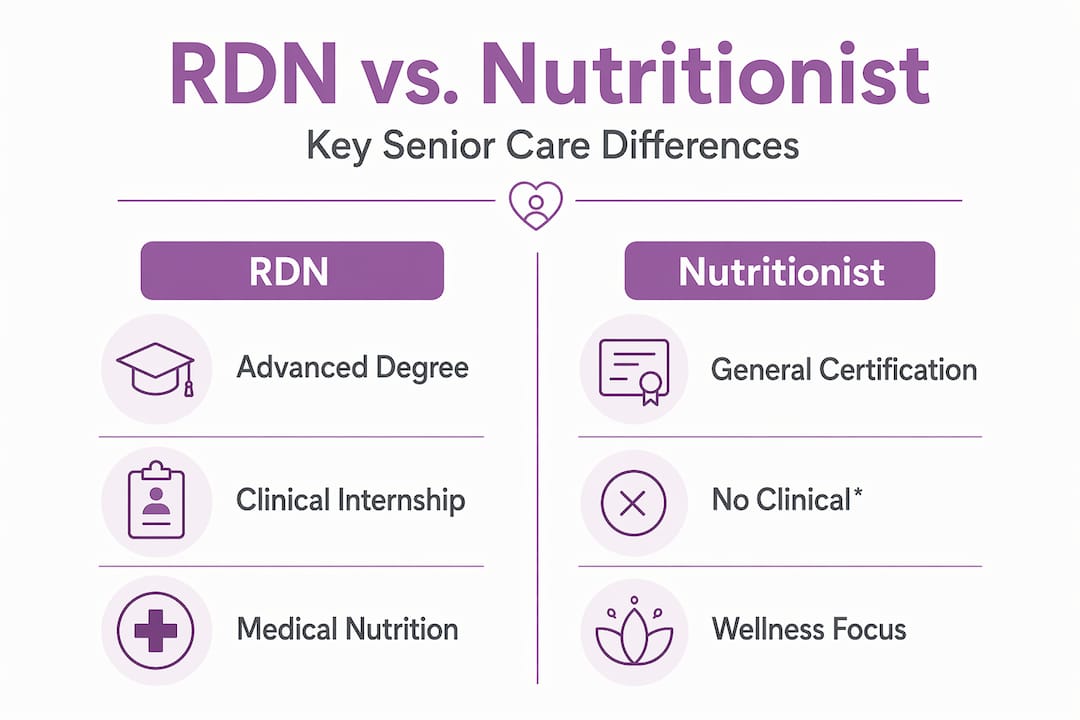
It is also worth understanding that Medical Nutrition Therapy is a specialized clinical service requiring a physician order. It addresses diagnosed conditions like diabetes, renal disease, and cancer-related malnutrition. It is categorically different from the community’s general dining program, even if both involve food.
| Service type | Provider | Requires physician order | Addresses diagnosed conditions |
|---|---|---|---|
| General dining program | Dietary staff, reviewed by RDN | No | No |
| Medical Nutrition Therapy | RDN (clinical role) | Yes | Yes |
| Texture-modified diet | RDN + kitchen staff | Often yes | Yes (dysphagia) |
Pro Tip: When touring any assisted living community, ask this exact question: “Does your RDN review individual resident nutrition assessments, or only the facility menu?” The answer tells you everything about the depth of clinical nutrition care provided.
Meals as social medicine
Nutrition in assisted living communities is not just about what goes on the plate. It is about who sits at the table.
Shared mealtimes improve seniors’ appetite, mental health, and reduce social isolation, all of which directly affect nutrition status. Residents who eat with others consistently consume more food and report greater satisfaction with their meals than those who eat alone. That connection is not trivial. It is one of the reasons structured dining programs in assisted living communities produce better health outcomes than home-based care where meals are often solitary.
The routine itself matters too. Fixed meal times create anchors in the day that support cognitive orientation, reduce anxiety, and give residents something to anticipate. For seniors with early-stage dementia, this predictability is therapeutic in ways that go beyond calories.
“For many seniors, the dining room is the most socially active space in the entire community. A missed meal is often not a dietary problem. It is a social signal worth paying attention to.”
The connection between nutrition, mood, and longevity runs deep. Seniors who eat well within structured communities show lower rates of depression, better immune response, and measurably longer lifespans than those with poor nutritional intake and limited social contact. Healthy eating in assisted living is, in part, a social intervention.
What families and caregivers should do
You are not powerless in this process. Families who stay engaged with their loved one’s nutrition care get better outcomes. Here is what that looks like in practice:
- Ask about clinical oversight: Confirm that an RDN reviews individual resident nutrition plans, not just the facility’s general menus.
- Understand therapeutic diet orders: Know what your loved one’s physician has prescribed and verify that the kitchen is executing it correctly.
- Watch for warning signs: Unintentional weight loss, low fluid intake, confusion, fatigue, or frequent infections can all signal malnutrition or dehydration.
- Track hydration actively: Use a daily hydration tracker or ask staff to log fluid intake if your loved one is at risk.
- Communicate food preferences: Facilities can often accommodate cultural or personal food preferences within therapeutic diet parameters. Ask.
- Visit during mealtimes: You will learn more about a community’s nutrition culture in 30 minutes at lunch than in a full formal tour.
Pro Tip: If your loved one is losing weight without an obvious explanation, request a formal nutrition assessment from the facility’s RDN rather than waiting for the next quarterly review. Weight loss of 5% or more in 30 days is a clinical flag that requires an immediate response.
Challenges in nutrition care that are rarely discussed
Even well-run communities face situations that do not have clean answers.
- Conflicting dietary restrictions: A resident with diabetes, heart failure, and kidney disease may have three overlapping therapeutic diets that create genuine conflicts. RDNs must prioritize and document trade-offs with physician involvement.
- Resident autonomy vs. safety: Residents have the right to refuse therapeutic diets. When that happens, facilities must document informed refusal and involve the physician when safety is at risk. Dignity and safety must coexist.
- Dysphagia mismanagement: Texture modification errors are more common than families realize. Serving the wrong consistency to a resident with dysphagia can cause aspiration pneumonia. Ask specifically how texture-modified diets are tracked and verified at kitchen level.
- Family-provided food: Well-meaning family members bring outside food that conflicts with therapeutic diets. This is a real problem facilities struggle to manage tactfully. Coordinate with nutrition staff before bringing anything.
- End-of-life considerations: At a certain point, aggressive nutritional intervention may conflict with comfort-focused care goals. These conversations require compassion and clarity from care teams and families alike.
Pro Tip: If your loved one has dysphagia, ask the facility to show you their IDDSI compliance process. A facility that can clearly explain how they train kitchen staff on texture-modified diet preparation is one that takes safety seriously.
My perspective on what families consistently miss
I have worked with hundreds of families going through the assisted living search, and I see the same blind spot repeatedly. Families assume that because a community has a dining room and a menu, nutrition is handled. It is not the same thing.
The difference between a facility where an RDN reviews each resident’s individual care plan versus one where a nutritionist glances at the weekly menu is the difference between clinical care and compliance theater. Both communities can say they have nutrition oversight. Only one is actually providing it.
What I have found is that families who ask sharp questions early, before placement, get better care. Not because facilities respond to pressure, but because asking those questions signals that you are paying attention. Staff remember which families show up at mealtimes and ask about weight trends. Those residents get more attentive care.
I also think the social dimension of nutrition in assisted living is almost always underestimated. The dining room in a quality community is a health intervention. Loneliness shortens life. Shared meals fight it. When you are evaluating a community, watch how the dining experience is designed. Is it rushed? Are tables set for connection or efficiency? Those details reveal the culture of the place.
Balancing clinical necessity with resident dignity is genuinely hard, and the best communities do it thoughtfully. Your job as a family member is to stay engaged, ask questions, and trust your instincts when something feels off.
— Eric
How Assistedlivingadvisers can help you find the right community
Choosing an assisted living community means evaluating dozens of factors at once, and nutrition programs are one of the hardest to assess from a tour alone.
At Assistedlivingadvisers, we help families across the New York, New Jersey, and Connecticut tri-state area find communities that meet both clinical care standards and quality-of-life expectations. That includes evaluating how facilities handle dietitian oversight, therapeutic diet compliance, and dining culture. If you are ready to start the search, explore assisted living options near you or learn more about how assisted living supports senior wellbeing. Our guidance is free, personalized, and built around what your loved one actually needs.
FAQ
What is the role of nutrition in assisted living?
Nutrition in assisted living supports physical health, cognitive function, immunity, wound healing, and social engagement. It includes both general meal programs and, when needed, clinical services like Medical Nutrition Therapy for diagnosed conditions.
How often should a Registered Dietitian review a resident’s nutrition?
At minimum, an RDN should review individual resident nutrition plans at care plan meetings, typically every 90 days, and immediately following any significant weight loss or health change.
What are signs of malnutrition to watch for in a senior?
Key signs include unintentional weight loss, fatigue, frequent infections, poor wound healing, confusion, and reduced appetite. Weight loss exceeding 5% in 30 days is a clinical threshold requiring immediate intervention.
What is the difference between a nutritionist and an RDN in senior care?
A Registered Dietitian Nutritionist holds an accredited degree, completed a clinical internship, and passed national board exams. The “nutritionist” title is unregulated in most states, meaning qualifications vary widely and clinical accountability differs significantly.
How does dehydration affect seniors in assisted living?
Dehydration in older adults causes urinary tract infections, cognitive fog, fatigue, and increased fall risk. Because seniors have a diminished sense of thirst, active hydration monitoring by staff is a critical safety measure, not an optional extra.
Recommended
Let’s Work Together To Find The Ideal Senior Living Community For Your Loved One.
Assisted Living Advisers is a FREE, personalized service offering expert guidance in determining the ideal community for your loved one based on physical needs, location preferences and finances.